
-
Acne Treatments
-
A procedure in which a chemical solution is applied to the skin to remove the top layers. The skin that grows back is smoother. With a light or medium peel, you may need to undergo the procedure more than once to get the desired results.

Deep Pore Treatment
A Deep Pore Treatment is a clinical procedure aimed at extracting comedones that occur in clogged pores and ultimately supporting your skin. This treatment helps to smooth skin texture and improve overall skin health.
Chemical Peel
Not all peels are created equal, and one peel type doesn’t suit all. That’s why certain ingredients may be more effective for treating hyperpigmentation, while others may be more successful in treating acne or addressing signs of aging. At Acne Clinic NYC, we offer light peels and power peels, depending on your skin concern and its severity.
Vi Peel
It is an advanced chemical peel designed for pigmented, aging skin and acne scars. By promoting cell turnover, it helps improve tone, texture, and clarity, revealing a more radiant, youthful complexion.
LED Light
LED (light-emitting diode) light therapy is a non-invasive treatment that enters the skin’s layers to improve the skin.
Aerolase
The Aerolase laser is a device used for an inflamed type of acne, post-inflammatory erythema, hyperpigmentation (post-acne marks) and rosacea. It utilizes patented technology to deliver precise, safe, and efficient care for all skin types.
Laser Genesis
Laser Genesis is a non-invasive laser treatment designed to rejuvenate, improve skin texture, reduce acne and promote a more even complexion. It effectively targets both post-inflammatory erythema and post-inflammatory hyperpigmentation. The laser stimulates collagen production, reduces inflammation, and improves skin tone for all skin types with none to minimal discomfort.
Excel V
Excel V is an advanced, non-invasive laser treatment designed for individuals looking to address a variety of skin concerns including redness, rosacea, and pigmentation.
AviClear
AviClear is the first and original FDA-cleared energy device for the treatment of mild, moderate and severe acne. AviClear specifically targets the source of the oily substance on your skin. After treatment, you will produce less oil, and your acne will get better and stay better.
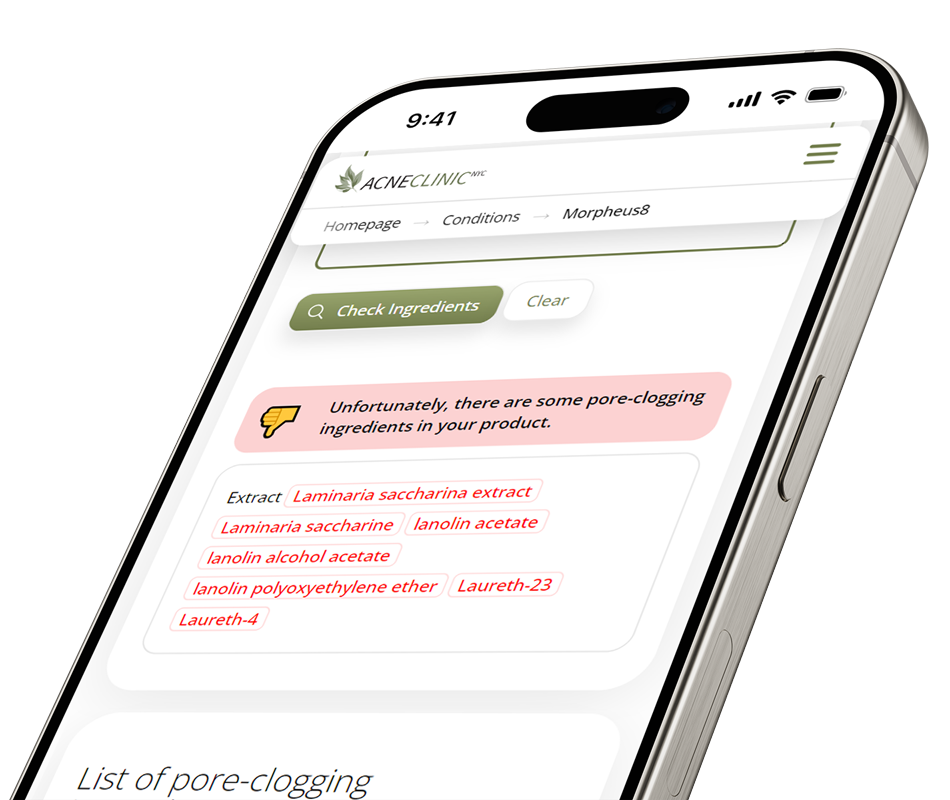
The world’s first and most trusted Pore Clogging
Ingredients Checker
Thousands trust us to deliver accurate, reliable analysis that empowers you to confidently choose skincare, makeup, and haircare products that support clear, healthy skin
Call You Back?
Share your phone number, and our client care team will contact you to answer any questions and help book your visit





